
African Safari Health Guide 2026: Vaccinations, Malaria & Medical Prep
Health Preparation for Your Africa Safari
Health preparation is one of the most practically important and most commonly under-researched elements of Africa safari planning. Most travelers spend hours comparing lodges, reading game drive reviews, and researching wildlife species. They treat health and medical preparation as a last-minute checklist item completed in a single pharmacy visit a week before departure. This approach works until it doesn’t. The consequences of inadequate preparation in a malarial destination can derail an entire trip. Arriving in Uganda without the yellow fever certificate that border control requires can do the same. The purpose of this guide is to provide the framework for thorough health preparation. It includes enough detail to make informed decisions at a travel health clinic and to arrive in Africa genuinely ready for the medical realities of the destination.
Africa safari health preparation has three distinct components that require different lead times. Vaccinations may require weeks or months before departure. Malaria prevention requires a prescription and a decision about which prophylactic to use. A medical kit and travel health insurance must cover the specific scenarios most likely to arise in the bush. Each component is different in kind and requires a different planning process. The travel health clinic consultation. Ideally scheduled six to eight weeks before departure — is the single most important step. It consolidates all three into a coherent preparation plan tailored to your specific itinerary and medical history.
Required and Recommended Vaccinations
What Your Clinic Will Recommend
Yellow Fever and Mandatory Entry Requirements
Yellow fever vaccination is mandatory for entry to Uganda, Rwanda, and several other African countries. Many African nations require it for travelers arriving from other African countries with yellow fever transmission risk. The vaccination produces a certificate. The International Certificate of Vaccination (the “yellow card”). That border control or airport health screening must receive at countries with mandatory requirements. The certificate is valid for life following the 2016 revision of international health regulations. Some individual countries still require evidence of vaccination within the past ten years, however. Border control requirements can also change without notice. The vaccine itself requires a minimum of ten days to provide protection. This makes it essential to vaccinate well before travel rather than immediately before departure.
Beyond yellow fever, a travel health clinic will assess your existing vaccination history and recommend boosters or new vaccinations based on your specific itinerary. Hepatitis A and typhoid are routinely recommended for travelers visiting areas where food and water hygiene standards vary. Hepatitis B is recommended for travelers who may require medical procedures or have other exposure risk. Meningococcal meningitis vaccination is recommended for travelers visiting the meningitis belt of sub-Saharan Africa, which includes parts of East Africa. Rabies pre-exposure prophylaxis is considered for travelers spending extended time in rural areas or with planned wildlife handling activities. Pre-exposure vaccination does not eliminate the need for post-exposure treatment but allows more time before treatment and reduces the total doses required. Routine vaccinations — tetanus, diphtheria, pertussis, polio, measles, mumps, rubella — should all be current before travel.
Timing Your Clinic Appointment
The six-to-eight-week lead time recommendation before departure allows enough time for vaccines that require multiple doses. Hepatitis B requires three doses over a compressed or standard schedule. It also provides the window needed for pre-exposure rabies vaccination. Which consists of three doses administered over 21 to 28 days. The yellow fever vaccine requires at least ten days to provide protection. It should not be given to immunocompromised individuals or certain other medical categories. These travelers require a medical exemption and alternative risk management strategy if the vaccine is contraindicated. Beginning the vaccination process earlier than six weeks is always preferable to beginning later. Travelers with complex medical histories or immunocompromising conditions should allow more time for their health provider to consult specialists if necessary.
Many countries offer online travel clinic booking services that allow travelers to specify their destination countries and receive a provisional vaccination recommendation before the appointment. Country-specific health advice is available from government public health agencies in the UK (TRAVAX, NHS Fit for Travel), the US (CDC Travelers’ Health website), and Australia (Smartraveller). All of these maintain regularly updated destination health profiles with current vaccination recommendations, disease risk information, and entry requirement details. These resources supplement rather than replace the travel clinic consultation. Travelers with any significant medical history should always discuss their specific situation with a qualified travel health physician rather than relying solely on web-based general information.
Malaria Prevention
Understanding Risk and Choosing Prophylaxis
Malaria Risk Across Africa Safari Destinations
Malaria risk is not uniform across Africa’s safari destinations. Understanding the risk level in each specific destination is the first step in choosing an appropriate prevention strategy. High-risk malarial destinations include Uganda, Tanzania, Zambia, Zimbabwe, Botswana (in northern areas during the wet season), Mozambique, and coastal Kenya. Moderate-risk destinations include the Masai Mara in Kenya and parts of Tanzania’s highlands. Lower-risk or malarial-free destinations include South Africa’s Cape Town and the Western Cape, the higher-altitude areas of Rwanda and parts of Kenya above 2,500 metres, and Namibia’s desert and coastal regions. The distinction between high, moderate, and lower risk matters because the choice of antimalarial prophylactic should be calibrated to the actual risk level rather than taking the maximum intervention regardless of destination.
The main antimalarial prophylactics available for African travel are atovaquone-proguanil (brand name Malarone), doxycycline, and mefloquine (brand name Lariam). Each has a different dosing schedule, side-effect profile, and cost. Atovaquone-proguanil is the most commonly prescribed for East and Southern Africa travel. It starts one to two days before travel, continues daily throughout the trip. And stops after seven days of leaving the malarial area. It has a low side-effect burden for most travelers but is expensive for long trips. Doxycycline is a daily antibiotic that also provides effective malaria prophylaxis. It is cheaper than atovaquone-proguanil and must begin two days before travel. It must continue for four weeks after return. Doxycycline can cause photosensitivity — increased sun sensitivity — which is relevant in Africa’s high UV environment. Mefloquine requires weekly doses and beginning five weeks before travel to confirm tolerance before departure. It associates with neuropsychiatric side effects in a proportion of users and should be discussed carefully with a physician before prescribing.
Non-Pharmaceutical Malaria Prevention
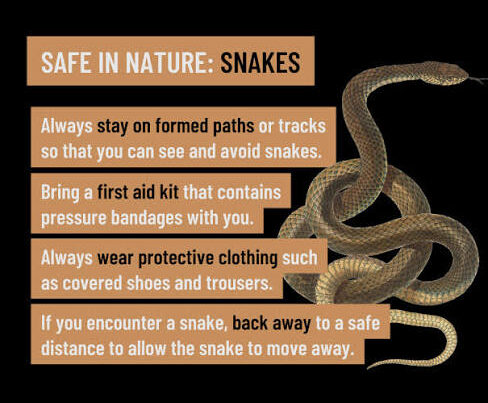
Antimalarial prophylaxis is most effective when combined with insect avoidance measures that reduce the number of mosquito bites received. DEET-based insect repellents applied to exposed skin at dusk and dawn. When Anopheles mosquitoes are most active — significantly reduce bite rates. Clothing covering arms and legs during the evening hours further reduces exposure. Permethrin-treated clothing provides additional protection and is particularly useful for travelers who spend extended time in the field. Sleeping under permethrin-treated mosquito nets in accommodations without air conditioning or fully sealed rooms eliminates overnight bite risk. Most reputable safari lodges provide well-sealed rooms, air conditioning, and bed nets. Budget travelers in public park camps or basic guesthouses should confirm the availability of nets and consider bringing a personal net from home if the accommodation standard is uncertain.
The most important message about malaria prevention is that no single measure is completely effective on its own. Antimalarial prophylaxis reduces risk but does not eliminate it. Insect avoidance measures are essential complements rather than alternatives. Travelers should also be aware that malaria symptoms can appear up to three months after leaving a malarial area. Returning home and stopping prophylaxis does not immediately end the risk period. Any fever developing within three months of leaving a malarial destination should be reported to a physician as potentially malarial. The possibility of breakthrough malaria, while uncommon, makes post-travel awareness as important as pre-travel prevention.
Medical Kit and Safari Travel Insurance
A basic safari medical kit should cover the common medical events that occur in the bush without immediate access to a pharmacy or clinic. Essential items include: a thermometer (for monitoring temperature in the event of fever). Rehydration sachets (oral rehydration salts for diarrheal illness and heat-related fluid loss). Broad-spectrum antibiotic (for traveler’s diarrhea if bacterial. A physician can prescribe this ahead of travel with appropriate guidance on when to use it); antihistamine tablets and cream (for allergic reactions and insect bites); ibuprofen and paracetamol (pain and fever management); personal prescription medications in adequate supply with copies of prescriptions; antifungal cream (for skin infections in humid conditions); blister plasters (essential for walking safaris); tweezers (for thorn and splinter removal); and a quality waterproof first aid guide. Travelers with specific medical conditions — asthma, diabetes, cardiovascular conditions — should discuss additional preparations with their physician before travel.
Travel insurance for Africa safari should specifically include medical evacuation coverage that extends to remote areas. Many safari destinations — the remote camps of Zambia, Tanzania’s southern circuit, Namibia’s desert parks — are more than an hour by air from the nearest surgical facility. In a medical emergency requiring surgery or intensive care, medical evacuation may be the only viable option. Policies that cap medical evacuation coverage or exclude coverage in remote areas are not adequate for safari travel in East and Southern Africa. The Flying Doctors Society of Africa (AMREF) operates medevac services in East Africa and sells annual membership that provides evacuation coverage for a flat fee. This is widely used by both residents and travelers in the region. South Africa’s ER24 and Netcare 911 operate comprehensive emergency response services throughout Southern Africa. Confirming the emergency contact numbers of the relevant service for each destination and storing them in your phone before arrival is one of the most practically useful pre-departure health preparations you can make.
Plan Your Safari
Health preparation begins with a travel clinic appointment six to eight weeks before departure. The single most important step in ensuring that vaccinations, prophylaxis. And medical kit are all correctly calibrated to your specific Africa itinerary. African Wild Trekkers provides destination-specific health information to all clients as part of our pre-departure briefing. This includes current vaccination requirements and malaria risk levels for each country on your itinerary.
We connect all clients with relevant health resources and medical contacts for each destination. We include flying doctor and emergency evacuation contact information in our pre-departure documentation. Every traveler arrives in Africa knowing exactly what to do and who to call in any medical situation.
Contact African Wild Trekkers at africanwildtrekkers.com/contact with your destination countries and travel dates and we will include full health preparation guidance alongside your itinerary design within 24 hours.